
Proposed NIH cuts may not stand, but renewed debate highlights the fragility of US geroscience funding at a pivotal moment for the field.
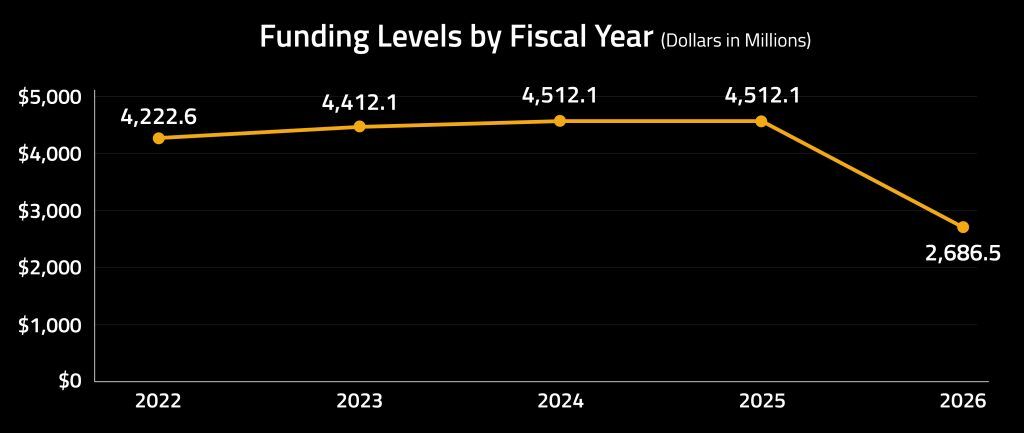
Earlier this year, the US administration’s FY 2026 budget proposal landed with an unhelpfully heavy thud in the biomedical research community; the suggested reduction in NIH funding approached 40 percent, with the National Institute on Aging facing a similar contraction. Although Congress has since indicated little appetite for cuts of that magnitude – and bipartisan voices have emerged in support of maintaining NIH appropriations – the proposal has nevertheless cast a long shadow. Laboratories, universities and research institutes depend on multi-year signals of stability; sudden, sweeping suggestions of austerity tend to travel fast, unsettling grant planning, career pathways and the confidence needed to pursue ambitious long-horizon science.
For those working in geroscience and aging biology, the discussion has resurfaced at a moment when the field is anything but quiet. New data types, in silico modeling, interest in senolytics and metabolic modulators, and emerging clinical work in biological age reversal have given the field a sense of acceleration. Momentum in prevention and healthspan research is building, yet the policy backdrop remains unsettled – and researchers are increasingly vocal about what that instability may mean.
Longevity.Technology: The prospect of deep cuts to NIH funding – even if now politically softened or heading for the legislative long grass – spotlights a growing mismatch between scientific momentum and financial commitment: the field is finally hitting its stride just as the fiscal weather decides to turn inclement. Aging is not merely another disease silo but the substrate on which almost every chronic condition is built; to pare back support for the very research that underpins healthier, more resilient societies feels economically counterintuitive – and strategically short-sighted. Policymakers may view budget tightening as prudent housekeeping, yet the returns on geroscience rarely arrive in neat, election-cycle-friendly increments – they crescendo over decades, reducing frailty, compressing morbidity and delivering savings that dwarf the initial outlay. Austerity at this juncture risks slowing not one project or institute but the entire preventive architecture required for an aging population.
Moreover, uncertainty itself is corrosive; laboratories that depend on multi-year stability hesitate to take risks, university cores delay hiring and early-career researchers who might otherwise commit to aging biology start eyeing up more predictable fields. The US has long been a gravitational center of longevity research, yet international competitors are scaling up precisely as the NIH contemplates scaling back – a timing mismatch that feels less like stewardship and more like self-sabotage. Fiscal discipline has its place, of course, but treating geroscience as discretionary rather than foundational overlooks the demographic reality bearing down on healthcare systems. If we genuinely want societies in which people live longer, healthier and economically productive lives, we cannot keep expecting prevention to scrape by on small change while disease treatment devours the notes.
Voices from the field
Several researchers have recently shared their unease on social media, not in reaction to the initial proposal alone but in response to what they view as a broader climate of uncertainty. Andrew Steele noted that if cuts of this scale were applied proportionally to the Division of Aging Biology, US federal support for longevity science would fall from “$1.04 per American to 62 cents” – a contrast that feels stark when set against the rising burden of age-related diseases. Jason Williams, MD, took a more clinical view, calling the moment “terrible timing” given emerging evidence for immune restoration, cancer–aging mechanistic overlap and early work in partial biological age reversal.
Through a broader lens, Nir Barzilai used a recent Medscape 2050 address to restate a view that has become increasingly mainstream: aging is “the mother of disease” and targeting its biology is a moral imperative. While he does not predict dramatic extensions of maximum lifespan, he argues that healthspan can be meaningfully lengthened and that, by 2050, younger adults may have access to interventions capable of reversing part of their biological aging. Such prospects rely on sustained investment in basic and translational research rather than short-term budgetary shifts.
Why indirect costs matter
Much of the early concern centered on indirect costs – the less visible but essential funding that keeps research institutions running. These reimbursements support laboratory maintenance, compliance, IT infrastructure and the administrative scaffolding required for regulated science. Cutting indirect cost rates may appear efficient, yet the reductions fall unevenly; research-intensive universities shoulder high fixed costs and rely on these funds to maintain safe, functional environments. Without them, institutions must either reallocate internally or reduce capacity – a choice that erodes the ecosystem on which longevity research depends.
Aging biology in the policy landscape
The National Institute on Aging funds a broad portfolio, from fundamental mechanisms studies to clinical trials and population-level research. Debate within the field remains nuanced: Max Unfried has suggested that much NIA-funded work does not directly advance efforts to halt or reverse aging, while João Pedro de Magalhães has argued that breadth is intrinsic to biomedical progress and that some of the most surprising insights – such as recent research on bowhead whale DNA repair – emerge from exploratory, curiosity-driven investigations. What both perspectives recognize is the importance of continuity; aging research depends on long-term cohorts, shared animal resources and infrastructure that cannot be switched on and off. There is shared acceptance that research requires stability; “more shots on goal”, as de Magalhães put it, are needed, not fewer.
These scientific considerations sit alongside wider demographic ones. Healthy longevity is increasingly central to economic and social planning – affecting workforce participation, healthcare budgets and the sustainability of public services. Public funding therefore carries a strategic weight: not because private capital is absent, but because foundational and long-horizon work rarely attracts the level of commercial investment needed to sustain momentum.
Signals and consequences
The proposed NIH cuts are not settled policy, and congressional resistance suggests that the most dramatic versions may never reach implementation. Nevertheless, the signal has been loud enough for advocacy organisations to mobilize. The American Federation for Aging Research’s statement earlier in the year stressed the need to protect early-career investigators and maintain a robust research pipeline, noting that even the prospect of contraction can reshape institutional decisions long before any budget is enacted. AFAR also urged policymakers to recognize the strategic value of aging biology, and its central argument – that progress in geroscience depends on continuity, not sporadic support – now reads as a prescient reminder of what is at stake.
A quiet inflection point
Regardless of where the FY 2026 appropriations ultimately land, this debate has shown how tightly scientific advance is coupled to policy stability; research thrives when institutions can plan with confidence and falters when uncertainty encourages caution. As societies age and the search for preventive strategies accelerates, the challenge may be not simply how to fund longevity science but how to ensure that investments keep pace with what the science is beginning to promise.

