
Antonio Bianco is a world-renowned physician-scientist and expert in thyroid physiology and metabolism. In this episode, Antonio explores the complex biology of thyroid hormone production, conversion, and regulation—highlighting how deiodinase enzymes modulate hormone activity at the tissue level and why that matters for interpreting lab results. He discusses the shortcomings of relying solely on TSH as a marker of thyroid function, the ongoing debate around combination therapy with T3 and T4 versus standard T4 treatment, and how genetics, tissue sensitivity, and individual variability influence thyroid hormone metabolism. The conversation also examines how hypothyroidism affects energy, mood, cognition, and longevity; why some patients remain symptomatic despite “normal” labs; and how future research could reshape treatment paradigms.
Timestamps: There are two sets of timestamps associated with the topic list below. The first is audio (A), and the second is video (V). If you are listening to this podcast with the audio player on this page or in your favorite podcast player, please refer to the audio timestamps. If you are watching the video version on this page or YouTube, please refer to the video timestamps.
How the thyroid produces, stores, and activates hormones like T4 and T3 to finely regulate thyroid activity [A: 2:45, V: 0:11]
- Galveston is 3 hours away, where Antonio is dean of the medical school and runs a lab
Tell me a little bit about what your research focuses on, and maybe even what got you interested in studying the thyroid system?
- Antonio’s research is trying to understand what thyroid hormone does
- And by understanding what it does in different tissues, we will be able to serve patients that don’t have sufficient thyroid hormone (patients with hypothyroidism)
- He focuses on the action of thyroid hormone at the tissue level: What does it do in the liver? What does it do in the heart?
- But then we go into the cell level, and we are currently looking at how thyroid hormone affects the folding of the chromatin
- Because that’s how it regulates gene expression
- Basically that’s how T3 or thyroid hormone acts: by regulating different genes
- And because the genes are basically the essence of the cell functioning, by regulating the expression of those genes, it changes the way the cell behaves, and that has an important consequence for the whole tissue, and for the organ, and for the body
Let’s start with the stuff that is largely known about the thyroid
- Many people know that they have a gland that sits over the voice box called the thyroid gland and that it produces a hormone
- Some people might know that the hormone is actually inactive ‒ it’s abbreviated T4, because it has 4 iodines on it
- And now we’re getting maybe past what most people would know, but enzymes in the body take 1 of those iodines off, and make an active form of that hormone that we abbreviate T3
⇒ Peter suspects that a number of people watching or listening realize that this hormone [T3] is very important, and it has properties that regulate energy expenditure, body temperature, mood, sleep, all sorts of things
- The final thing that is probably common knowledge is that it is not entirely uncommon that some people don’t seem to make enough of that hormone for one reason or another, and that as a result of that they have to supplement that hormone
- And that condition could be referred to as hypothyroidism
- We’re going to talk about all of these things, of course
- Peter would venture that there are tens of thousands of people listening to us right now that would identify as having hypothyroidism, and that are taking some form of thyroid replacement
Our objective today is to make sense of this whole thing, because there are so many different ways that people think about how to replace that hormone, there are so many different that people think about how to diagnose the condition, and it seems that it is a much more complex endocrine situation than the other major systems we think about
- It doesn’t seem very difficult to understand what low testosterone is
- You have a very simple assay, you understand the symptoms quite well
- Replacing it is quite simple
So, with that said, let’s go back to that meta-level, layer on as much detail as you’d like about the thyroid gland and what it’s doing
- That was a great introduction
- The thyroid gland, what it does is takes up iodine from the blood and uses that iodine to produce a hormone
- That’s quite interesting, quite unique
- We basically ingest iodine every day on our diet (for example, seafood is full of iodine), and we really need that iodine so that the thyroid can function
⇒ Without iodine there’s no thyroid hormone. Luckily, what we do is we supplement the kitchen salt with iodine.
- This is not something that we have to worry, if you have a reasonable amount of iodine every day, it will provide sufficient amounts to make the thyroid hormone
- The thyroid traps iodine, and through a series of complicated reactions it makes up the thyroid hormone
- It also stores a large amount of hormone
⇒ The thyroid is basically a large storage of thyroid hormone, mostly the pro-hormone, the inactive hormone, T4
- T4 has 4 atoms of iodine
- The thyroid slowly secretes T4 into circulation on a daily basis so the blood has a storage of T4
⇒ Now, T4 doesn’t do much, when we talk about the importance of thyroid hormone, it’s important for the brain, important for the heart, for the bones, we’re not talking about T4, we are talking about the other hormone, the active hormone, T3
- It’s amazing that by just removing one atom of iodine from the T4, it now becomes a fully active hormone
- And why is that?
- Because cells, tissues, have receptors
- The receptors don’t like T4, they don’t bind T4 that much
- Receptors love T3, they bind T3 with high affinity
Peter asks, “This is just purely a conformational difference or is it electrostatic?”
- It’s conformational, it doesn’t fit into the pocket of the receptor
- The pocket of the receptor has low affinity for T4 ‒ if you put a lot of T4 then yes, you’re going to get some action, but normally those are extremely high levels
From an evolutionary perspective (not that we can ever know for sure), do you suspect that the reason for this is that it makes more sense to secrete an inactive pro-hormone that has a long half-life that can go everywhere and then each tissue can selectively make its determination of how much active hormone it needs?
- The evolutionary pressure is iodine deficiency
- The whole system evolved in a way to preserve iodine
- You see, the thyroid is full of thyroid hormone, it has 4 atoms of iodine, and then by removing one, it becomes active
- So, it’s preserving iodine as much as possible
- And what happens with that iodine that was removed?
- It’s taken back up again
It’s all about preserving the iodine so that we don’t go into a situation that we don’t have enough iodine to produce that hormone
Presumably when iodine is abundant, you can stockpile more T4 within the gland
- Absolutely, that’s right
T3 is the active hormone
- Once you remove the atom of iodine, what happens is that the molecule becomes T3 (the active hormone), but then it has a short half-life
⇒ The contrast between T3 and T4 is dramatic: T4 has a half-life of about 8 days, T3 has a half-life of about 12 hours
- Once T3 is activated, it triggers its destruction
- It has a brief action
- It works potently, however it’s targeted for destruction (it’s just metabolized and cleared)
- And that tells you that this is a way the body has to regulate the action of thyroid hormone
- So, once it’s activated, let’s make sure it’s still active 12 hours later (you still need to have all that activity)
- It slowly activates, and if for any reason we have to stop activating, after you stop, shortly after the action of T3 will decrease
That’s a way of limiting the amount of exposure of the tissues to the active thyroid hormone
Peter has heard that there are different deiodinases
- Just for the listener, the deiodinases are enzymes that (as its name suggests) remove an iodine atom from T4 to [create] T3
- Correct
But there is a molecule called reverse T3, say a little bit about that and how it differs from T3
- Reverse T3 is AT3, an alternative form of T3
- It all depends on which iodine is removed from the molecule of T4
- The molecule of T4 has two rings, the inner ring and the outer ring [shown in the figure below]
- If you remove the iodine from the outer ring, you make T3 [T3 is on the left side of the figure below]
- If you remove the iodine from the inner ring, you make reverse T3 [rT3 is on the right side of the figure below]
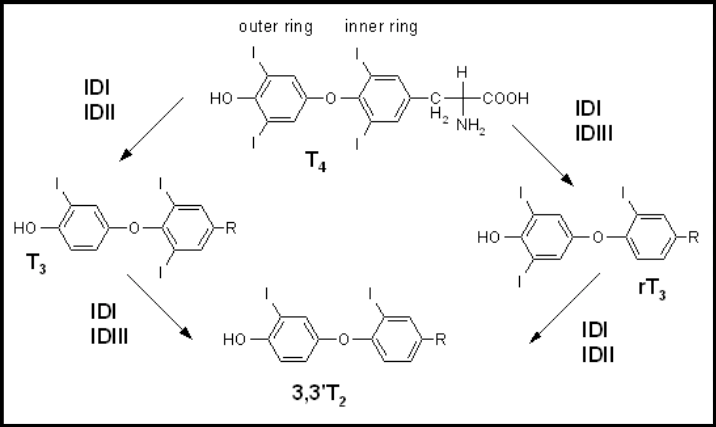
Figure 1. Synthesis of T3 and reverse T3 (rT3) from T4, and synthesis of T2. Image credit: Wikipedia
Peter asks, “Does it matter which one from the inner ring and which one from the outer ring?”
- No, it doesn’t
- Either one can do the trick
- And the amazing thing is that, whereas T3 is a super active molecule, reverse T3 is dead, it has less activity than T4 even
- You really need an astronomical amount of reverse T3 to do anything to the receptor (so, it’s really not active)
The thyroid is constantly secreting T4 into the circulation
- The deiodinases will take T4 and either make T3 or reverse T3
- And so, either activates or inactivates thyroid hormone
- And that constitutes an alternative pathway that can also be altered on a moment’s notice
- For example, all of a sudden you have all this T4 available, and let’s say the body wants to reduce the activation of thyroid hormone
- Instead of putting the T4 through the T3 pathway, T4 will preferentially go through the reverse T3 pathway and will be completely inactive
How fasting alters thyroid hormones to conserve energy [A: 12:45, V: 11:08]
A very extreme case, but a true scenario
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.

